Physician compensation 2023: The good, the bad, and the ugly

Let's face it: Physician pay in 2023 was a mixed bag, at best. Doctor salaries edged up, but gains were overshadowed by rising inflation. Against the backdrop of the pandemic, a doctor shortage, pay inequities, burnout, and unionization, healthcare systems must recognize that fair compensation is the crux of attracting and retaining doctors. But there's no one-size-fits-all solution.
This is the first in a series of MDLinx doctor compensation reports, drawing upon the most current data from the Medical Group Management Association (MGMA)—gleaned from nearly 190,000 practitioners—along with other sources. We'll unpack the complex factors that affect physician pay and their impact on doctors, their patients, and public health.
The state of doctor compensation
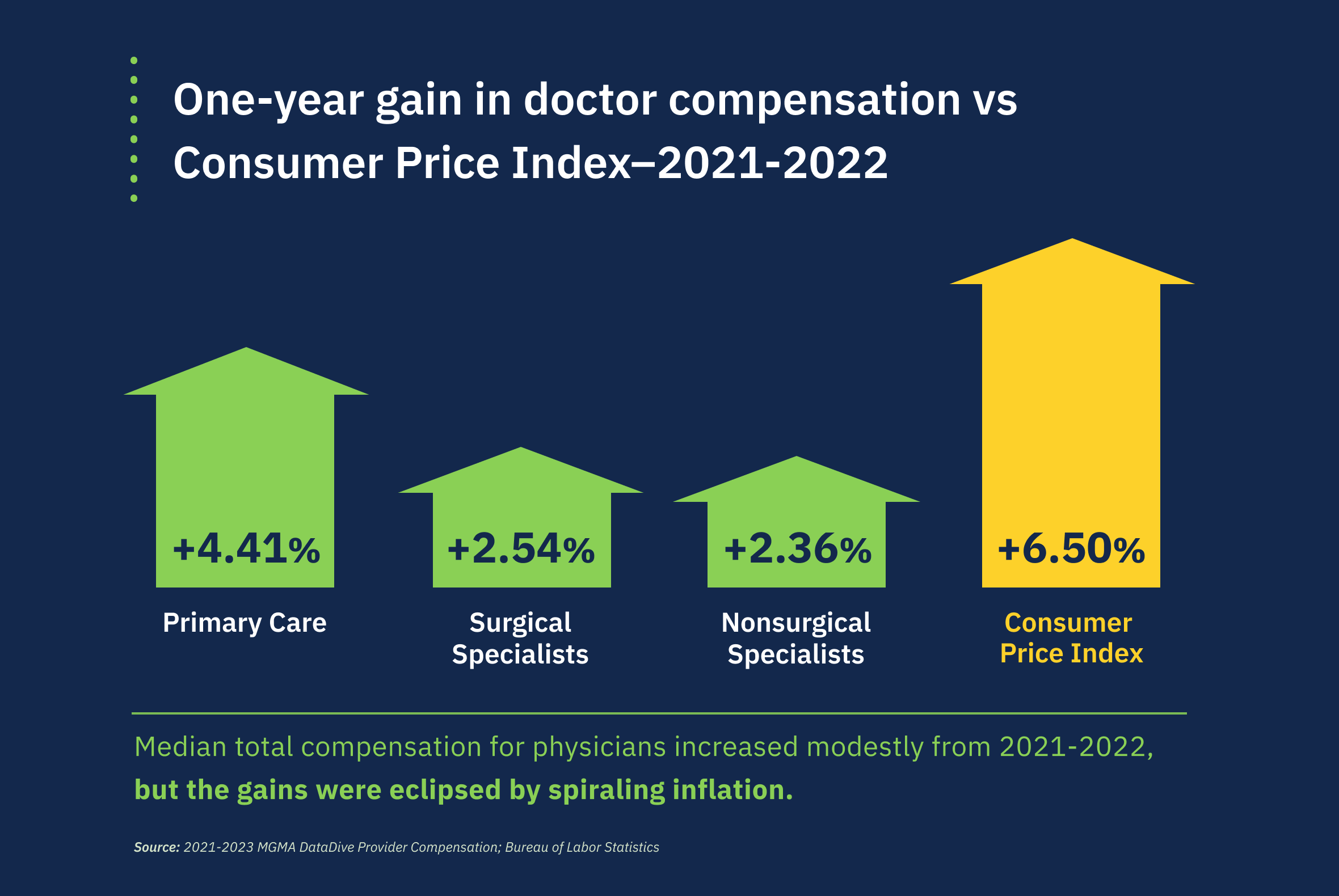
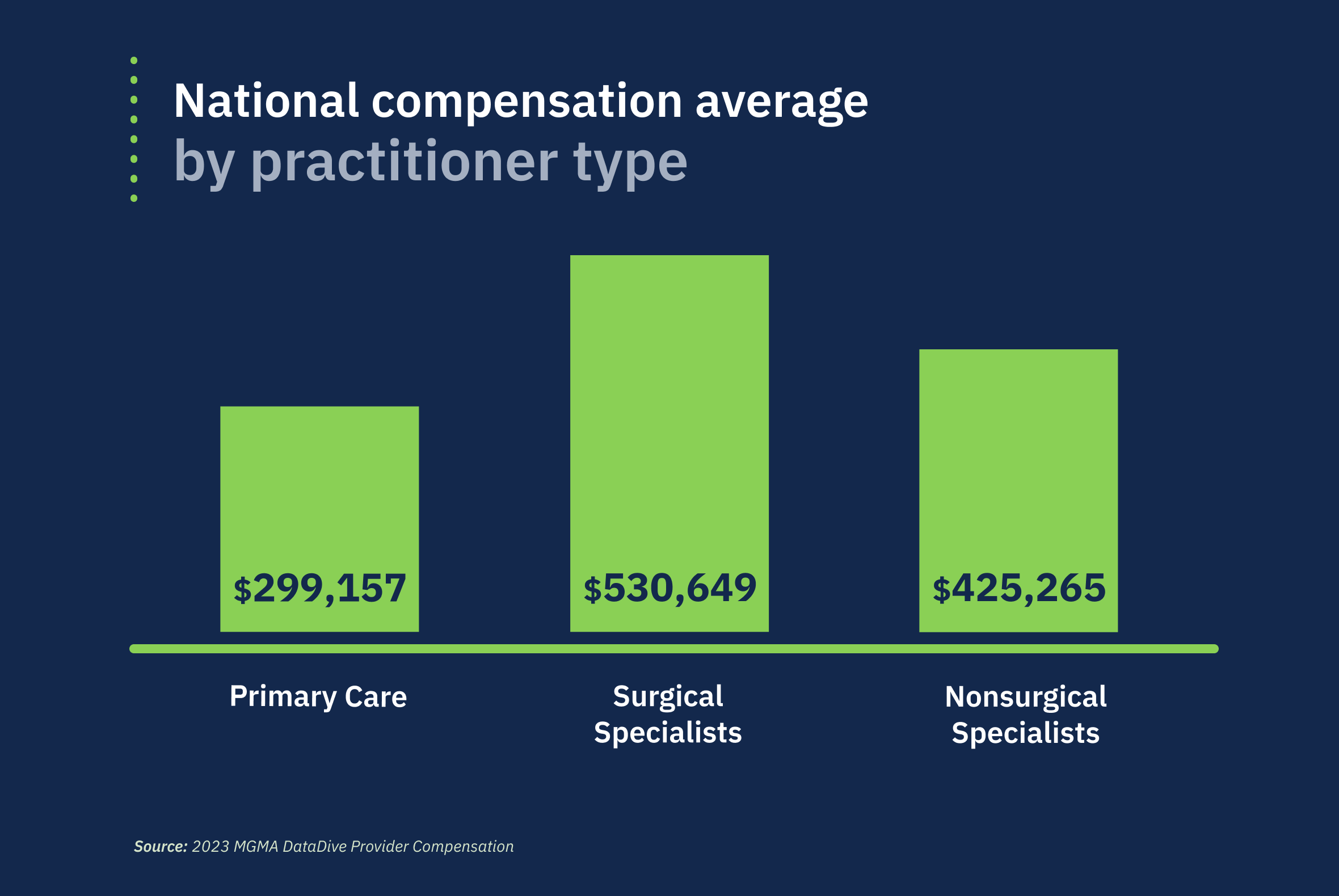
According to MGMA's 2023 physician compensation report (2022 data), primary care practitioners (PCPs), surgical specialists, and nonsurgical specialists all saw modest growth in compensation from 2021 to 2022.[1] PCPs fared the best, with their median total compensation growth doubling from 2.13% to 4.41% that year.
But those gains have not kept pace with the nation’s inflation rate—the Consumer Price Index shot up 6.5% from 2021–2022, according to the US Bureau of Labor Statistics.[2]

The reasons for this mismatch are multifactorial in nature, as physician compensation is dependent on many variables, among them:
Experience and tenure
Medical specialty
Geographic location
Regional healthcare market conditions, including demand
Facility (eg, academic medical center, outpatient clinic, ambulatory care unit, etc.)
Practice ownership and group composition
Relative value units (RVUs)
Physicians must also navigate state-by-state differences in reimbursement rates and malpractice laws.
Also adding to the equation: Primary care, as a rule, has quality control measures that limit the cost of care, while specialists/surgeons provide more expensive services that drive up the cost of care. Both PCPs and specialists are working in concert to manage patient costs and maximize health outcomes—despite inadequate staffing and lack of resources.
While the above trend is consistent across the country, physician pay is not, with the largest discrepancies related to practitioner type and where services are rendered. Let's look at the numbers.
Pay by specialty and geographical area
Which specialties earn the most? That number can vary, depending on whether compensation figures include salary, bonus, profit-sharing contributions, and the like. But according to Medscape's 2023 physician compensation report,[3] the top five highest earning specialties (based on full-time salary only) are:
Plastic surgery: $619K
Orthopedics: $573K
Cardiology: $507K
Urology: $506K
Gastroenterology: $501K
These same top-earning specialties have held steady over the past decade, Medscape notes.
As for pay growth, oncology saw the biggest boost in compensation (13%), followed by gastroenterology (11%), with anesthesiology, radiology, critical care, and urology all seeing 10% growth.
Specialties on the low end of the pay spectrum, according to Medscape, include: public health/preventive medicine ($249K); pediatrics ($251K); family medicine ($255K); infectious disease medicine ($262K); and diabetes and endocrinology ($267K).
By region
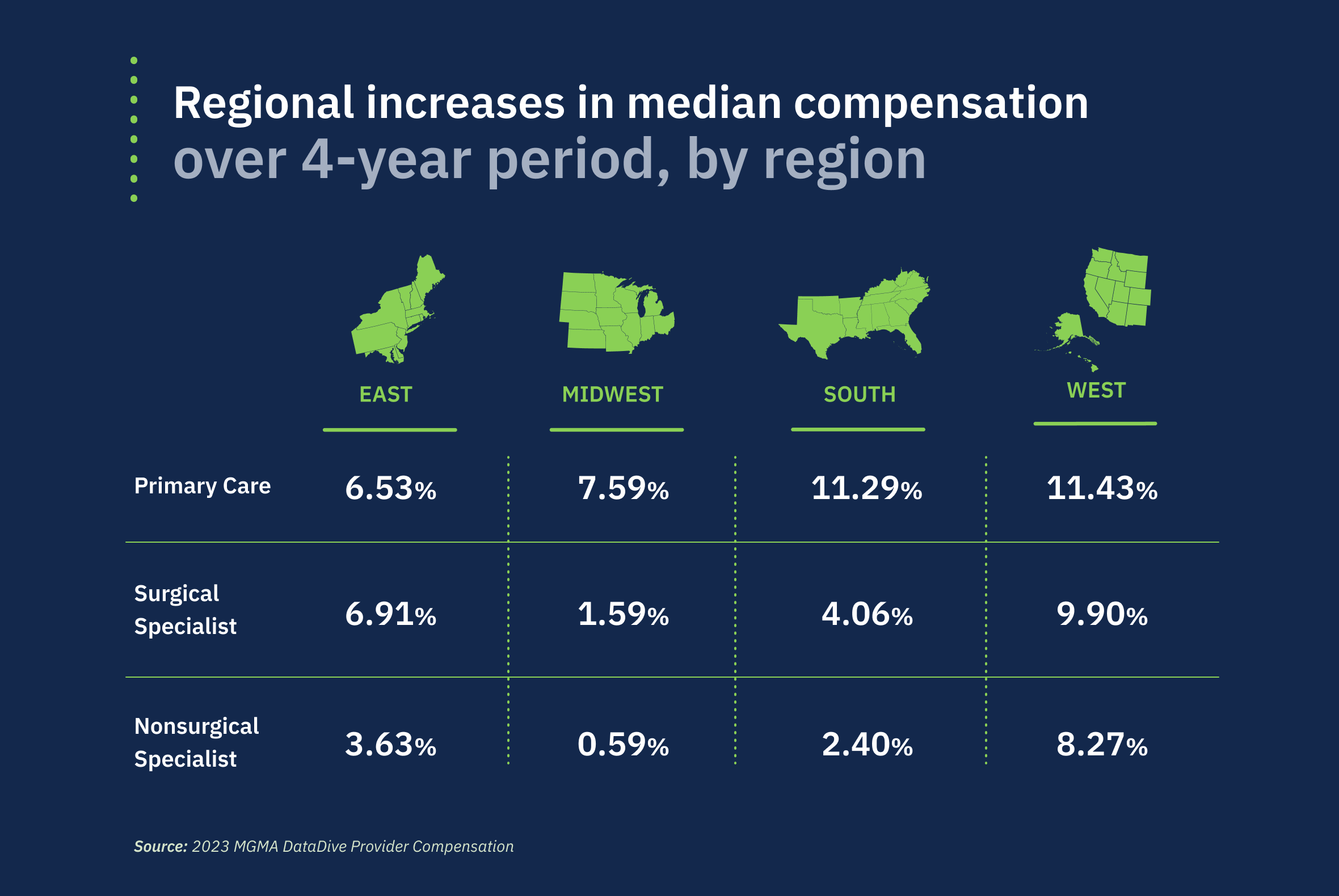
Geographic location is one of the major determinants of physician pay. And according to MGMA's data, physicians in the West have experienced larger increases in total compensation over a 4-year span (from 2019–2022) across all fields—primary care, surgical, and nonsurgical—than other areas of the country (East, Midwest, and Southern regions).
Calvin Lambert, MD, an OB/GYN who specializes in Maternal Fetal Medicine at The Mount Sinai Hospital in New York City, thinks demand is one of the primary reasons for these differences.
"In places where it’s difficult to recruit physicians, like rural areas such as South Dakota, employers figure their only way to entice physicians is with higher compensation."
— Calvin Lambert, MD, The Mount Sinai Hospital, New York
“Metropolitan areas that are more heavily populated are often more desired by physicians, many of whom come from those environments, so naturally hospitals and physician groups don’t have to offer the same packages as their rural counterparts,” Dr. Lambert tells MDLinx.
Does that mean that rural doctors have more money in their pocket at the end of the day? It's not that straight-forward. While the differences in physician salary between rural and urban work settings may seem stark, differences in cost-of-living expenses and state taxes narrow the gap substantially. New doctors, or any physician who is job-seeking, will want to take this into consideration in their employment search.
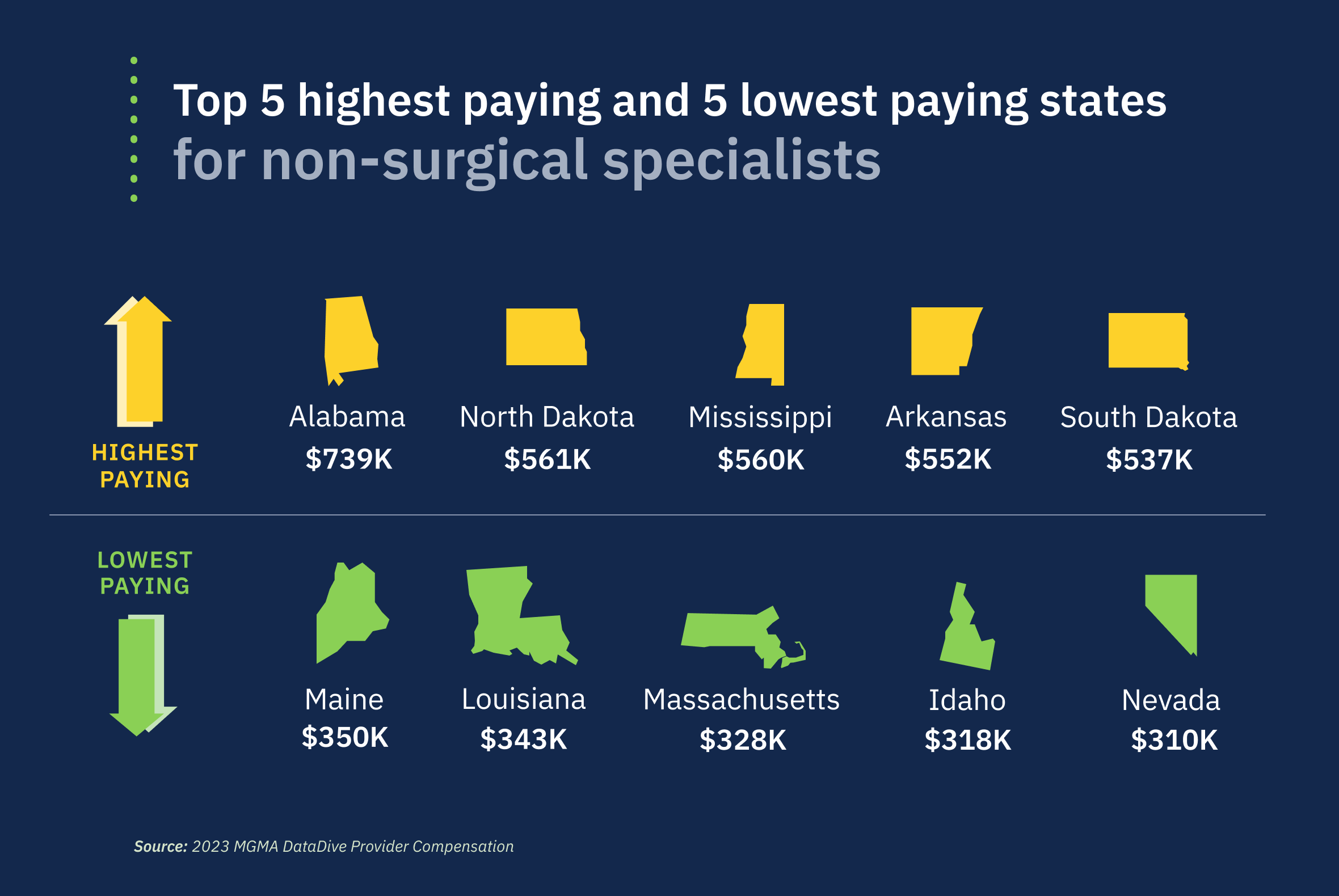
By state
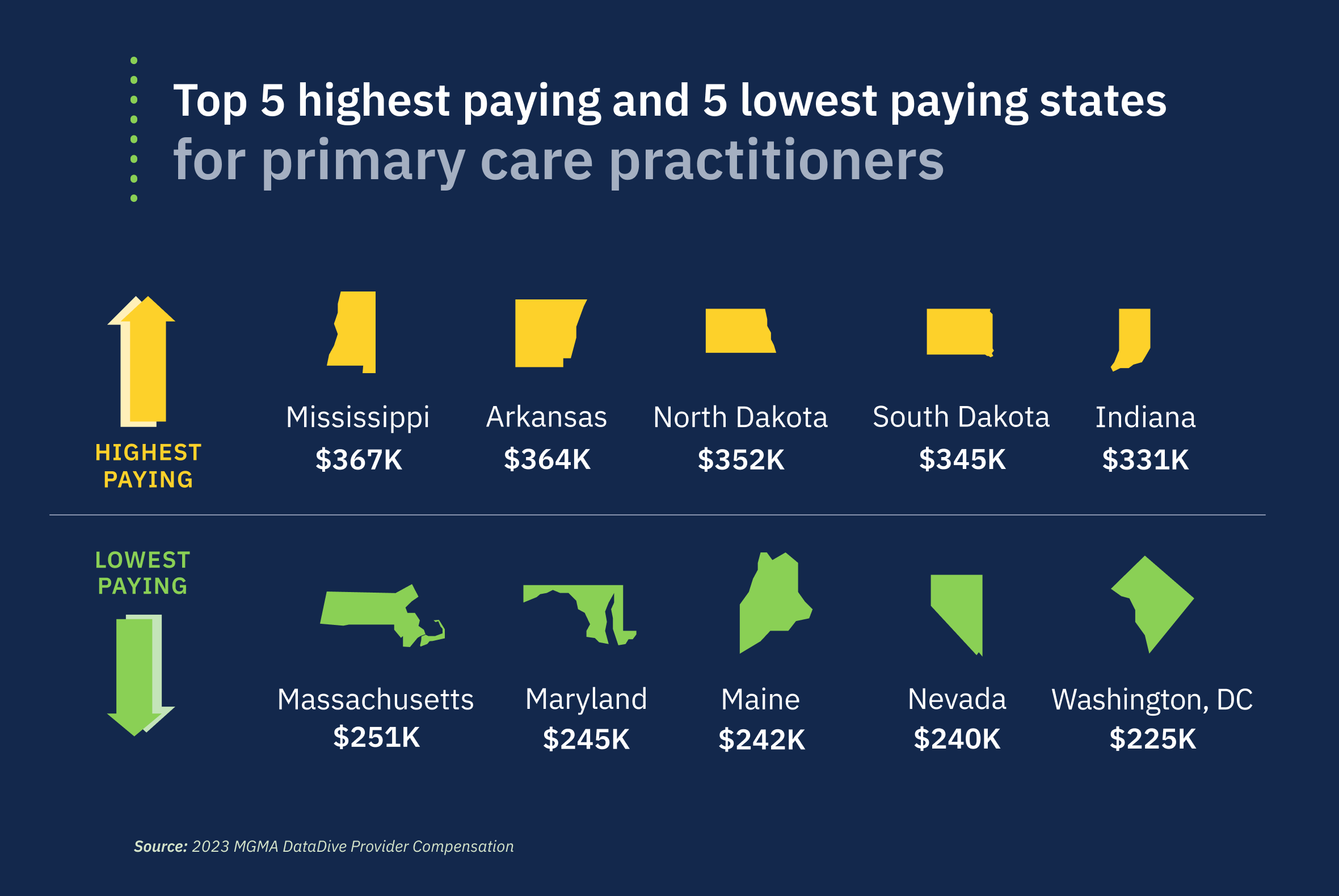
The differences among physician pay across specialities from state to state are staggering, even taking into account higher cost-of-living expenses and taxes in more urban areas.
Primary care physicians in Mississippi earn nearly $140,000 more on average than their lowest-earning counterparts in Washington, DC, according to MGMA data.
The regional differences in surgical and nonsurgical specialist pay are even greater, with surgical specialty physicians earning $327,000 more in South Dakota than their lowest earning counterparts in Louisiana. Nonsurgical specialty physicians earned over $400,000 more in Alabama than their lowest earning physician counterparts in Nevada, per MGMA.

Unpacking the issues
Complex compensation packages
Physician compensation is complicated in large part because there's no universal physician pay model that works for everyone.
Some strides have been made, thanks to a shift away from managed care—a healthcare delivery system made popular in the 1990s, which created extremely complicated pay models for doctors. But complexities remain, and in some cases have worsened due to the COVID-19 pandemic.
The pandemic exposed the flaws of traditional fee-for-service payment models, as many US hospitals and health systems saw their revenue streams dry up when non-emergency services were deferred and volume-based services stopped.
As more physicians turn to unions as a means to protect their compensation and worker rights, healthcare systems are recognizing the importance of pay and benefits in attracting and retaining talented physicians, which improves job satisfaction and patient care.
But designing fair compensation models for employed physicians has become more challenging as the number of payment models and auxiliary compensation factors, such as Medicare reimbursement, staff shortages, personal performance, and quality metrics, has grown.
A 2023 MGMA Stat poll points to the slow adoption of value-based care throughout the industry, nudging more medical groups toward incorporation of quality metrics in their comp models.[4] According to the poll, 47% of medical groups tie quality performance metrics to physician compensation plans, vs 53% that do not.
Misperceptions about doctor salaries
Are doctors overpaid? Some people think so, because on average, physician salaries are higher than for any other major US profession, and they are far higher than for doctors in other countries.[5]
But many argue to the contrary, saying that's an unfair assessment based on an incomplete picture.
For starters, most US doctors graduate with high debt, face high malpractice insurance premiums, and are starting families and careers at the same time. These financial obligations make fair compensation essential.
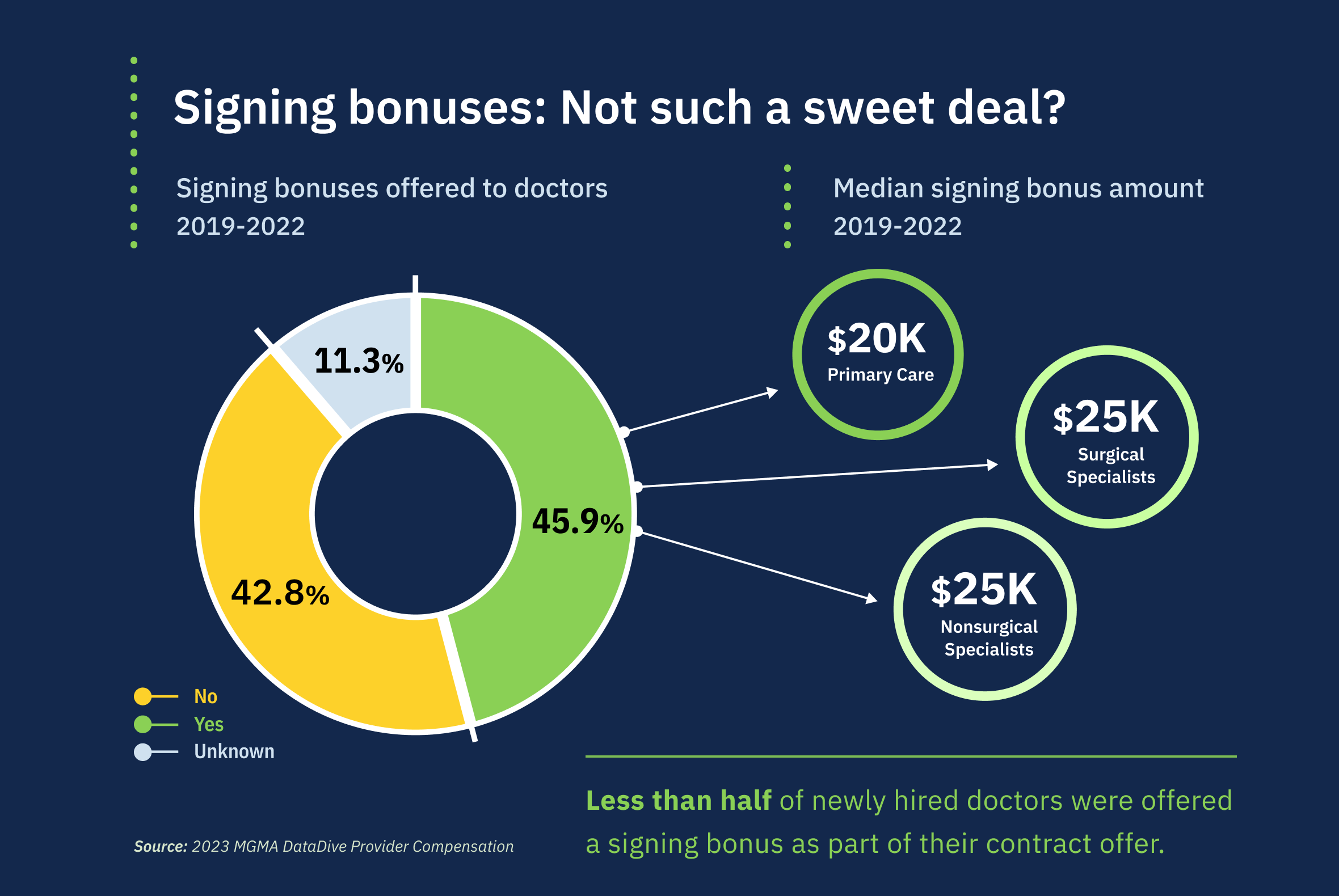
And these days, physicians are also less likely to get “sweeteners"—ie, signing and starting bonuses or other incentives—in their contracts, according to MGMA data.
Still, high salaries are a function of supply and demand, partially due to need and market pressures. For example, the national physician shortage encourages employers to offer competitive salaries, not only because it's a way to attract a scarce entity, but also to make the medical field more desirable. Steep decreases in compensation would exacerbate the shortage in the short and long term.
The doctor shortage
Physician shortages are a nationwide problem, with rural areas more affected than metropolitan areas. Burnout is a major contributor, as doctors are often overworked and burdened with clinical and administrative stress.
To attract and keep doctors, medical systems offer higher wages and better benefits. This reaction is commensurate with the laws of supply and demand—as demand for a good or service increases, so does its price. Fittingly, as the demand for doctors, especially PCPs, increases, so does their pay.
But there is a cost: Increased pay can lead to higher procedural costs, which are often passed on to patients.
Pay disparities
Pay inequity based on gender and race remains a thorny issue in medicine—a relic of systematic disenfranchisement, according to an AAMC report on medical school faculty salaries.[6] Salary equity conversations have primarily focused on the gender pay gap without addressing equity issues more broadly, the authors noted.
"Greater attention should be paid to potential salary inequities by other demographic variables, such as race/ethnicity and sexual orientation, as well as gender identity."
— Authors, AAMC faculty salary equity report
Studies show that gender pay gaps are gradually decreasing, but there is still much room for improvement. A 2023 study published in JAMA Health Forum underscores this point with its examination of marriage, children, and sex-based differences in physician hours and pay.[7]
Researchers analyzed data on more than 95,000 physicians between 2005-2019, and found that female physicians bring in less income than male physicians, regardless of age or family makeup.
"Male physicians earned 21% to 24% more per hour than female physicians across all family structures," the authors wrote. "Marriage and children were associated with an additional earnings penalty for female physicians, which is primarily due to fewer hours worked relative to male physicians."
For physicians with children, the male-female disparity in pay over a 40-year career exceeded $3 million, more than double the gap for single physicians.
While most studies point to gender as the primary factor driving pay inequities in medicine, Black, Indigenous, and people of color (BIPOC) consistently experience inequitable pay compared with their White counterparts. According to Medscape, White physicians earn almost $50,000 more annually than Black physicians—$358,000 vs $311,000, respectively.
Dr. Lambert believes that overt and covert forms of racism are the reason. “Social constructs have historically assigned, albeit erroneously, values to certain groups that remain part of the institutional framework among the healthcare systems in the US,” he says.
He notes that bias, and the fact that women are nearly twice as likely to go into primary care specialties as men, play a role in wage disparities. “These fields are notoriously under-compensated comparatively to profit-driven, procedural-based modalities that offer higher compensation,” Dr. Lambert says.
All of these factors are compounded by the “minority tax paradigm,” a burden of time and resources placed on minority persons to represent and advocate for their communities in the workplace, says Dr. Lambert.
“The minority tax is a real thing. BIPOC individuals who are dedicated to mission-driven work and creating opportunities for people who look like them often have their efforts perceived as extracurricular, and not as significant as, say, research from their colleagues,” Dr. Lambert explains. “Therefore, they’re forced to allocate their precious time to uncompensated and undervalued administrative work.”
The effect of RVUs on compensation
RVUs are a measure of the cost of doctor's services and procedures, and are tied to Current Procedural Terminology (CPT) codes—and they're important, especially for those whose salary is heavily dependent on Medicare reimbursement.
Medicare bases RVUs on the following three factors:
Physician work: This includes the doctor's knowledge, skills, and experience, plus the time and effort they spend performing a service, including documenting the patient's case and details of the service in the EHR.
Practice expenses: These include the costs of running a medical practice, such as staff salaries, rent, and equipment.
Professional liability insurance: These are the costs of insuring against the risk of lawsuits.
RVUs are a vital component in calculating physician compensation, as they standardize the value of medical services based on complexity and time. Knowledge of RVUs is essential for physicians as they directly impact reimbursement rates, influencing overall earnings and incentivizing efficient and high-quality care.
Practice ownership is also an important variable in calculating RVUs—a make-or-break component to physician compensation. MGMA data shows that physician-owned practices reported higher levels of productivity in collections, total encounters, and work RVUs compared with their hospital-owned counterparts for 2022. Total encounters reflect the number of direct provider-to-patient interactions regardless of setting, including televisits and e-visits.
The bottom line
Although salaries have recovered somewhat in the past few years, doctors still worry about pay, especially given their high debt loads—and this is magnified by ongoing pay inequities.
While higher salaries may help, better work-life balance is also essential. This can be addressed through measures such as adequate staffing, shorter shifts, more paid time off, and better parental leave policies.
Without these? We're likely to see the ongoing consequences of burnout, early retirement, and other negative impacts on the medical profession.
Read Next: Oncologist compensation 2023: High salaries, heavy debt, and burnoutExplore our Money Matters Rx series!
Want to boost your financial know-how? Grasping money management basics is crucial for doctors—from handling student debt, to running a practice, making investments, and saving for retirement. Check out MDLinx's Money Matters Rx series for doctor-specific advice on making smart financial choices at every career stage.
Sources
Provider Compensation. An MGMA Data Report. Benchmarking for the Future of Your Physician & APP Workforce. May 2023.
U.S. Bureau of Labor Statistics. TED: The Economics Daily. Consumer Price Index: 2022 in review. January 17, 2023.
Kane L. Medscape Physician Compensation Report 2023: Your Income vs Your Peers’. Medscape. April 14, 2023.
Nearly half of medical groups tie physician compensation to quality performance. MGMA Stat poll. May 16, 2023.
Frellick M. European Doctors Paid Half as Much as US Counterparts. Medscape. October 11, 2023.
Promising Practices for Understanding and Addressing Faculty Salary Equity at US Medical Schools report. AAMC. 2019.
Skinner L, Yates M, Auerbach, D, et al. Marriage, Children, and Sex-Based Differences in Physician Hours and Income. JAMA Health Forum. March 24, 2023.